The Last Witness
Kolya is lying in a cellar. The only thing separating him from the bare earth is a bit of Styrofoam to protect against the cold. The walls are moldy, the air icy and damp. Kolya wears two pairs of pants on top of each other, two pairs of socks, a cap and he’s wrapped in a blanket, he will later recall. And yet he’s still freezing. It’s March in Mariupol, and temperatures are dropping below zero.
There’s no more electricity and no water. No safety. Barely any food. The Russian army has surrounded the city, and now it is starving the population. Bombs rain from planes, Kolya can even hear them in the basement. A whistling noise followed by a tremendous thunder. The walls tremble as if he were lying in a house of cards that could collapse and bury him at any instant. A bullet recently hit the neighbor’s house and a man died. They buried him in the vegetable patch. They didn’t dare go any further because of the fighting.
Kolya’s sister Polina, 11, is lying next to him in the basement. She snuggles up to her father Vladimir, a slender, serious man. Polina is the youngest of the three children. Varya, 14, lies at Kolya’s feet. Next to her mother Natalia, whose corpulence keeps her warm. Between them is Kolya, who has just turned 17 years old.
He’s not religious, but he is praying right now. In his mind, he will later recall, he speaks the same sentence over and over again: Everything will be alright, we’ll get through this. But he doesn’t really believe what he’s saying. Kolya is certain he’ll die in Mariupol. And his family with him.
Before February 2022, Kolya had been a teenager who had discovered his love for Metallica and dreamed of changing the rigid Ukrainian school system as a civil servant. His sisters Polina and Varya were fond of folk dances and painting. Parents Vladimir and Natalia, both 47 years old, sometimes lacked the energy for three children. But after many conflicts during puberty, Kolya was growing closer to them again.
Today, six months after the start of the Russian war of aggression, they are dead. Polina and Varya, girls with long braids and high cheekbones, were likely killed by debris in the basement of their home. Vladimir, the father, died in the apartment, perhaps he had gone upstairs to get some air. The body of their mother still hasn’t been found to this day, presumably her body got pulverized by the explosion.
The only one still alive is Kolya, a child from whom the war took everything: his home, his family, his future and even his past. He no longer has anything except a pair of jeans and wool socks knitted by his mother. Kolya’s clothes, his identity papers, the people he loves – all these things lie under the rubble of Mariupol. Just like the other tens of thousands killed by Russia in its campaign against Ukraine.
A few days after the invasion in February, the Russian army cut off the city’s connection to the outside world. The network collapses, and it’s not a coincidence. The world isn’t supposed to see what is happening in Mariupol. To this day, there are few images from the city, and Russia has dismissed the ones that do exist propaganda.
But Kolya witnessed what happened in Mariupol. He is able tell you about it without hesitation or faltering, as clearly and distinctly as only someone who has nothing left but their story can. To corroborate his account, DER SPIEGEL spoke to Kolya’s former neighbors and friends. Videos and satellite images provide proof of the destruction of his childhood home. But only Kolya can still report about his family. He says he owes it to them to speak out about what happened. If he couldn’t save them, the world should at least be told how they died.
“My family is from Mariupol, but I was born in Donetsk, on December 19, the day of St. Nicholas. My parents named me after him: Kolya. They had to wait nine years for a child. The fact that they were able to then have daughters gave my parents great joy.
Dad worked in a steel factory and Mom was an accountant. They worked like slaves. Together, they earned 23,000 hryvnia a month, about 600 euros. It was enough for a small house. Varya and I shared a room, Polina slept with Mom. Dad slept on the sofa in the living room.
He was on shift duty and often had to work at night. He was always tired. Dad and I fought over little things, like the fact that I was supposed to do more to help around the house than my sisters. Today I think: how silly.
In the end, though, I would say the relationship in our family was ideal. All the problems seemed to have dissolved. Maybe also because I had grown up and become more serious. I could understand my parents and sisters better. Our lives had just begun.”
On February 24, a Thursday, Kolya wakes up to go to school. He’s still in bed when, half asleep, he hears his mother tell the girls in the room next door that class has been cancelled. Putin has declared war on Ukraine.
Many people in Mariupol still believe they’re safe. They believe that the troops won’t harm them. Putin allegedly wants to protect the Russian-speaking population with the attack, and it would be hard to find a Ukrainian city that is more Russian than Mariupol. More than 90 percent of the residents speak Putin’s native language in everyday life. Many feel closer to Russia than to Ukraine.
Kolya’s parents count among those people. They grew up in the Soviet Union, they speak Russian with their children and they stay out of politics. Their only desire is a modest, worry-free life. They hardly cared at the time whether that be under the Russian or Ukrainian flag.
During the first hours of the war, Kolya’s family, whose last name will not be used here to protect Kolya’s identity, buys food, but they don’t flee. They wouldn’t even know where to flee to. They’re simple people without relatives or relations abroad. Kolya never left Ukraine before the war. The family decides to ride out the Russian attack like it’s a thunderstorm.
As Kolya and his parents wait in line in the few supermarkets that are still open, the Russian army draws a ring around Mariupol. Already in the first hours, Putin’s military had shelled residential buildings and a school. Nevertheless, three quarters of the inhabitants remain in the city. They trust their “brother people,” who are pretending to protect them.
Kolya’s family is holed up in their building, a one-story structure on a quiet side street. The parents get out games for the children, and Vladimir, the dad, watches “Lord of the Rings” on TV. The shelling is still far away, and they can still tell themselves that the war isn’t affecting them. Kolya leafs through books he would otherwise have no time for because of school. He gets caught up in George Orwell’s “1984,” a story about a country turning into a totalitarian surveillance state. Between explosions, Kolya thinks about how much the plot reminds him of Russia.
“In the early days of the war, we even had online classes. There were explosions outside, but the teacher was talking about how we should do our homework. Everyone believed the Ukrainian army would be able to hold out in Mariupol. That it was only a matter of time before everything would return to normal.
One evening I was watching Star Wars with my friend Vika, with each of us as our own computer. Vika and I know each other from school, we have been a couple for two years. Her family also stayed in Mariupol. We lived only 10 minutes from each other. Visits weren’t possible, but we shared our screen on Skype and watched TV together.
Suddenly, the picture froze and the sound stuttered. I said: Vika, I can’t hear you anymore. Then there was a bang outside, sparks flying in the sky. The power went out.”
The Russians cut more than a dozen power lines in the first weeks of the war. After that, the only things providing warmth were the open fires many lit on their balconies. By now, at the latest, the residents of Mariupol are coming to realize that Russia has deceived them. But it’s too late. The way out of the city is already mined and blocked.
“It was freezing cold at home. We wore four sweaters on top of each other and also wrapped ourselves in blankets. It didn’t help, it was always cold. And then, just when we thought things couldn’t get any worse, the water disappeared.
At first, it was still dripping out of the tap. At some point, though, nothing came at all. That was the beginning of the apocalypse – I don’t have any other way of describing it. We lived like savages. We could no longer wash, and instead of a toilet, we used a bucket or plastic bags. To get water, we had to leave the house and go up the street, where there was a spring. The path was dangerous and the water was dirty. We boiled it over the fire. But it still tasted terrible.”
In the beginning, the family still lives in the house, they sleep in their beds and eat at their table. Although the rumblings of war are approaching, their dad initially refuses to prepare the basement as a shelter.
Each family member is confronting the threat differently. Kolya’s dad Vladimir with stoic denial, his mother Natalia with concern for her children. Polina, the youngest, is overcome by nervous hysteria: Instead of crying, she laughs herself silly all the time. Kolya, for his part, shakes uncontrollably, and he is no longer in full control of his hands and legs. He can barely sleep at night out of fear he won’t live to see the morning.
Then a shell strikes their neighborhood for the first time. Screeching, it flies over the building before dropping on its target with a bang. The ground shakes like an earthquake, Kolya feels it too.
The Russians destroy a gas station located only 200 meters away. Why, Kolya asks, would you fire on a gas pump? Russia, he says, explaining the attack, doesn’t even want to leave a few liters of gasoline for the population.
After the attack, the family does move into the basement, which is barely 1.70 meters high. They usually store canned cucumbers and tomatoes here, supplies for the winter. But it has now become the place where they sleep. They find some Styrofoam panels in the garage that they had bought to insulate the house. They lay them on the ground and place all the blankets they can spare on top of them. They only go upstairs to fetch water or to cook on the fire.
Kolya hates the basement. The walls are covered with mold, and there’s barely enough room for the family. But it muffles the sound of the carpet bombing of the city.
“The building shook with every impact. Dust settled on my face. I used to be ashamed of getting close to my parents, but now I wanted to be as close to them as I could. I took turns hugging my Dad’s and Mom’s shoulder, telling them I loved them.
Every day, I was prepared to die – even if I couldn’t understand what for. I was lying in the basement, listening to the explosions and wondering: Why was I brought into this world in the first place? Will I ever accomplish anything to be remembered by? Or if I die now, will it be as if I never even existed?”
Kolya, a child of 17, utters these sentences with the seriousness of an adult. During hours-long interviews with DER SPIEGEL, he doesn’t cry once – he doesn’t even sound accusatory. He just talks about what happened to him, and sometimes it seems as though he’s surprised anyone actually cares.
In the second week of March, Kolya remembers, a Russian rocket hit the building next door. And then further buildings on the street. When the bricks burst from the heat of the explosions, the sound penetrates all the way down into the basement. When, in a quiet moment, Kolya steps out onto the street, the asphalt in front of his door looks as if it has been dug up.
Kolya’s building is also slowly succumbing to the war. A blast wave damages the roof and the windows burst. The chandelier in the living room crashes down, along with part of the ceiling. At one point, an explosion is so powerful that parts of the kitchen walls bury the basement hatch. It’s only with a little luck that the family are able to dig themselves free.
It now just feels like it will only be a matter of time before they die. There are few search teams left in Mariupol. People who are trapped – and there are many – are rarely rescued. People are dying in their basements, in their living rooms, in a school and in the theater where hundreds of people seek refuge. Ninety percent of all buildings in Mariupol are damaged during the war. Anyone who has seen images of the bombing, of rockets indiscriminately launched at the city, inevitably wonders how anyone could survive here.
Vladimir, Kolya’s father, presses himself against the farthest basement wall day and night and stares into space. Kolya’s mom is no longer able to calm the children. Once, she wants to stroke her son’s cheek, whisper to him that everything will be all right, but when Kolya feels his mother’s hand, he collapses. Natalia’s skin is scratchy like sandpaper, scraped up from the debris. She notices his defensiveness and bursts into tears. “Is it my fault our building was bombed?” she cries. Then they cry together, mother and son, both helpless and vulnerable. This moment burns itself into Kolya’s memory – he still remembers every detail months later.
When the Russian shelling subsides somewhat, Kolya musters up his courage. He hasn’t heard from his girlfriend Vika in two weeks, he doesn’t even know if she’s still alive. He decides to take the 10-minute journey to her home to see she she’s doing.
Kolya’s home, part of a quiet residential neighborhood, had seemed especially safe to him at the beginning of the war. But Vika lives in a 14-story building, visible from far away – an ideal target for the Russian army. When he arrives at Vika’s building, it’s almost unscathed.
Of course, there’s no guarantee the people will survive here either. Here, too, people are buried in the yard; and here, too, residents are running out of food. But maybe, Kolya thinks, it would make it easier for him if he lived with Vika for a while. His family would have more room in the basement and one less person depleting the supplies. Vika’s parents agree.
“When I went back home, I said: Mom, I’ll probably move in with Vika. We were totally crammed into the basement. She agreed.
I packed a few things. Then I wanted to say goodbye. I don’t remember what my sister Polina was doing at that moment, but Varya was sitting in the basement, crying. She had always been strong, but she could no longer handle it. I stroked her head and tried to comfort her: We’re going to make it, everything will be OK. Please don’t cry.
When I was almost out the door, I turned back to my father. I said: Dad, I’m leaving now. He had been in a state of shock for days, lying on the floor and breathing heavily. Dad sat up, looked at me and said: ‘Well, go.’ It was the last time I saw my family alive.”
On March 10, Kolya moves from his parents’ house to his girlfriend Vika’s apartment. Meanwhile, the third week of the Russian war of aggression is raging. The first mass grave is dug in Mariupol. On March 13, the municipal government reports that the last water and food supplies have been consumed.
Vika’s family prepared and have supplies. They stored pasta and grits, and even the gas tank in the kitchen is still filled. Kolya can hear the impacts here, too, but at least he is no longer crouching in the cramped basement, but in a windowless hallway, the safest place in the apartment.
Vika, now 16 years old, seems lively and bubbly, Kolya serious and composed. They both like Nirvana and astrology, wear dark clothes and have a penchant for mysticism. They pass the time by talking about the war: What are the odds that Russia will win?
But it’s a useless endeavor: There has been no mobile phone network and no news for weeks. They can only guess the course of the front. Instead, Kolya and Vika consult their tarot cards. Vika pulls the card with a man standing on a hill, his gaze fixed on a sea full of ships. They conclude that a fleet will come to save Mariupol.
The reality, though, is that Mariupol is falling, district by district. In mid-March, there’s a sudden knock at the door of Vika’s apartment, with a man’s voice demanding in harsh Russian: “Open up! This is an inspection!” Putin’s soldiers are standing at the doorstep. They search the rooms and threaten to take the men away. Kolya is too young for them, and Vika’s father happens to be out looking for food. The Russians are combing all the floors, and shots are fired on one of them. Later, a neighbor tells Kolya that two bodies have been carried out to the street.
The Russian army now controls Vika’s neighborhood, and the shelling shifts to the southwest, where Mariupol’s main military unit, the Azov regiment, is still resisting. The fighters have retreated to the local steel factory, and Kolya’s family lives nearby. When he looks out the window, he sees Russian tanks being refueled and then driving off in the direction of his parents’ house. Kolya says he feels like he was a traitor. As if he had abandoned his family.
That’s also why he decides to stay in Mariupol when Vika and her parents leave the city. Since Russia has control of large parts of the area, it’s possible to get to Crimea. On March 21, his girlfriend gets into the car and drives off. Kolya stays in their apartment on his own.
“When everyone was gone, I burst into tears. I thought: What do I do now? Would it have been better to go with them? But I wanted to wait until my parents showed up. I was sure they would come for me at some point. And then I wanted to be there so they wouldn’t have to worry.
It wasn’t easy living alone in the building. The gas had since run out. I had to cook with fire and I had never done that before. Fortunately, a neighbor helped me. A family that had stayed in Mariupol lived a few floors above Vika. The man’s name was also Kolya. One of his sons spotted me on the balcony trying to make myself something to eat. He told me how to do it, and they also gave me some food later.
One night, it was March 24, I dreamed about my parents. I saw my father standing in the yard of our building. He had no arms left, as if someone had chopped them off. I screamed: ‘Dad, Dad, what have they done to you?’ Then I woke up. I didn’t know what the dream meant.”
The next day Kolya asks a neighbor to accompany him to his parents’ house. It’s a potentially deadly journey because of the fighting, but he wants to see how his family is doing. By now, all the remaining residents know the boy who lives alone on the fourth floor. The neighbor, a devout Christian, agrees to go with Kolya during a a break in the shelling. They say a last prayer and then they set off running.
They head in the direction of the Prospect of Metallurgists, a central avenue that was leafy during more peaceful times and filled with neon signs. Now buildings are shot up, trees have fallen and street lights are strewn all over the place. There isn’t a human in sight.
The first streets in Kolya’s neighborhood give him hope: The homes are battered but not destroyed. He sneaks around mines left by the army along the way. Finally, he’s standing in front of the gate to his house.
At first, he thinks: everything as usual. Then he looks again – and realizes that his parents’ home is no longer standing. Meter-high chunks of stone are piled up where the dining room once stood, the ground is churned up like a field. Bricks are lying on the wood, the ground and on pieces of furniture. Kolya’s home, the place where he spent his whole life, looks like someone ran it through a meat grinder.
“I looked at the ruins and didn’t grasp what had happened. I called for Mom, for my Dad, for my sisters. I ran around the house looking for the basement hatch, trying to squeeze through the rubble to them. But it couldn’t be done, it was too tight.
Suddenly, the neighbor said: ‘Kolya, look, there is a piece of clothing or a toy. What is that?’ I looked, it really looked like clothing, perhaps with fur trim. I moved closer and realized: It was Dad. He was lying face down, most of his body buried. Only his hands and head stuck out. His eyes were squeezed shut, his nose broken. He looked as if he had aged decades.
I began to dig for him with my hands. I was certain: If I managed to get him out, he would get up and run. But then I touched him with my fingers and his body was completely cold and hard. My Dad no longer felt like a person, but like a bag of dirt.
I lost it. I screamed, I cried. I yelled that I loved him. That I was sorry because I didn’t say goodbye the way I should have. Because I really thought this war wasn’t going to hit us.”
In the days that followed, Kolya tried to shovel his family out with the help of neighbors. One helper recorded the rescue attempts on a mobile phone: You see people pressing against the concrete with spades and metal rods. They couldn’t do it. Only an excavator could lift the debris. And there have been no excavators to dig out people buried in Mariupol for a long time.
Videos of a rescue attempt like this are also a rarity. In Mariupol, where there is no electricity, most mobile phones are out of juice. But a neighbor in Vika’s apartment building deals in electronics and happens to have a solar panel. He regularly charges his phone on it and films what is happening around his building. Dozens of recordings document the Russian siege. One of them shows Kolya standing in the ruins of his parents’ home, his face frozen with shock. As he and the neighbors try to make their way to the basement, loud bangs can be heard above them.
“I didn’t know what to do. I wanted to look for my mother and sisters, but I thought: If we stay here any longer, I’ll wind up getting us all killed. And even if we make it to the basement, the chances that Mom, Polina and Varya are still alive are slim. People in the other buildings said the rocket hit our house on March 17. That was more than a week ago.
I squeezed through the rubble with a flashlight, almost to the basement. The hatch was slightly open. I called out, but no one answered. I saw that there were bricks in the entrance to the basement. I couldn’t see any people.
I briefly held out hope that maybe Mom and the girls weren’t in the house when it was hit. That they had gone to church to pray or something. But I also had to realize that this was unlikely. If Dad was in the house, then Mom and my sisters were there too.
I realized that we would not find them alive. And that we had to stop digging for them so we wouldn’t die as well.
I wish I had come sooner and brought them over to where I was staying. I could have saved them. I felt so guilty.”
Kolya returns to his parents’ house only once after that. He has a homemade sign with him: a peg, broken from the door of an abandoned daycare center, along with a piece of wood he found. He writes the names of his family on it with a black felt-tip pen: Vladimir. Natalia. Varya. Polina. Born between 1974 and 2010. Died on March 17, 2022.
Kolya takes a brick and hammers the sign into the ground in front of the destroyed house, as a message to the Russians, who have since also taken control over this part of the city. They will begin removing the rubble, and they should know that there are still people under the concrete. Kolya hopes that they will dig up and bury the bodies of his family. But probably, he thought at the time, they would throw them away like garbage.
After Kolya puts up the sign, he once again sees his father lying among the rubble. The sun is shining over the city now, spring is getting closer. The bodies are starting to decompose and Kolya can smell it.
He climbs over the debris of his family home looking for something to cover his father with. Amidst the rubble, he finds a green down jacket that belonged to his sister Varya. There’s a video of it: Kolya asked his neighbor to record the impact site. He doesn’t want anyone to be able to claim later that he made all this up.
It shows Kolya throwing the jacket over the corpse of his father. He looks for a second garment in the rubble and places it over Vladimir’s head. After that, he leaves the destroyed building and walks away, perhaps forever.
Why did Kolya’s family have to die? According to international law, civilians are given special protection in war. But no price was too high for Russia’s army to conquer Mariupol. The soldiers shelled residential areas and hospitals, escape routes and shelters. It was intended to make Mariupol residents feel unsafe wherever they were. It looked like chaos, but it was calculated hell.
A hell that Kolya has been left to deal with alone. His family is dead, his hometown destroyed. A young man left to cope with this catastrophe on his own. He spends three days in Vika’s apartment: He remembers crying, beating the floor with his fists and convulsing. There’s still no electricity, no water, barely any food. Kolya knows he can’t survive without help.
The neighbors living a few stories above him turn out to be his salvation. The father of the family, who share’s Kolya’s name suggests: “Move in with us. We’ll take care of you.”
“His son had once helped me to make a fire and his wife told me how to boil noodles. Otherwise, I barely knew the family. But the man immediately said: ‘You no longer have a father, so I will be like your father. We won’t leave you alone.’
He and his children were there when we tried to dig out my family. They were the worst moments of my life, and they experienced them with me. That brought us closer together. I also had no choice: I had no one and nowhere to go back to.
The fighting in Vika’s neighborhood ceased in April, but everything was destroyed. No one knew if civilization would return in a month or in a year. So, the family that had taken me decided to leave Mariupol. They had a few cans of gasoline on hand and two cars that were riddled with shrapnel but still roadworthy. We left on April 18.”
From the windows of the car, the buildings they drive past look like Armageddon. Entire sections of the city are burning, cars are shot up and turned over. Kolya remembers an “atmosphere of death,” with mines lying all over the road. And his fear of not surviving as they escaped. But they make it to the front line, the border between Russian-occupied territories and Ukraine.
In the town of Manhush, the family waits for a week in a line of cars of the people fleeing. Hundreds are waiting for Russia soldiers to conduct checks on their cars. When the time comes, many men are taken away, but Kolya and his neighbors are lucky. Because they have Ukrainian and Russian citizenship, the soldiers wave them through. Kolya, the teen in the back seat, goes unnoticed.
He only remembers some of the rest of the trip. He no longer knows how he found out about their destination, nor how they got the to border with the European Union. Nor how the officials waved him through even though he has no identification papers – they burned in Mariupol. He only knows that he arrived in early May in a country he had never heard of. A green and quiet place, surrounded by mountains. We are not publishing the exact place where Kolya lives in order to protect his privacy.
Since July 2022, Kolya has been living in a refugee shelter, with six people sharing a few square meters. The family with whom he fled Mariupol lives there with him. It’s cramped, but Kolya is happy he’s not alone. The conversations with his rescuers keep him in the present, like an anchor that prevents the past from sweeping him away.
He calls it “losing touch with reality,” and it happens to him a lot. When it does, he no longer sees the meadow in front of his house or the blue sky, but instead the ruins of Mariupol. The worst, Kolya says, is when he lies awake at night. He then stares at the ceiling above his bunk bed, and in his eyes, the room becomes the basement where his family died.
“I miss Dad most of all, maybe because I saw him dead. I remember how he laughed and how I hugged him. He was very warm and soft. Later, when I found him, he was so cold.
What were Dad, Mom and my sisters thinking at the moment of the explosion? Did they have time to realize that this was the end for them? Did they feel fear? I imagine what it would have been like to be with them. Then I get scared.”
Mariupol has been fully under Russian control since May 20. There’s still no water in many places, and residents collect it from puddles using buckets. Dead bodies aren’t recovered by search teams, but by volunteers who receive food in return. Some young men have recently been forced to do military service and fight against Ukraine, their own country.
Kolya knows this – he follows every report from the city. On the only table in his room, there is a laptop that is almost always showing the news. He manages not to let the reports get to him too badly. People who have experienced trauma often compartmentalize what they have experienced afterward, and perhaps this explains Kolya’s composure. There are two Kolyas: The one who lies awake at night thinking about death. And the one who tries to look ahead so that he doesn’t break.
Kolya is now attending six-hours a day of language school. He bought himself a guitar, and the seller even gave him a discount when he heard that Kolya was Ukrainian. He spends his free time doing homework and dealing with the bureaucracy of his new country. And with Vika, his girlfriend, who against all the rules of probability is with him again.
He calls her just before he leaves Mariupol. He tells her that he’s alive and that he loves her – then the connection breaks off. The next time they talk by phone, Kolya has already reached Western Europe.
Vika’s family is living in Crimea at this time, but they don’t want to stay there. On the phone, Kolya asks her to come to him. Vika agrees. At the end of May they fall into each other’s arms at the train station, and there’s a video of that moment.
Vika now lives with her mother in a hotel rented for refugees from Ukraine. It’s located just a few streets away from Kolya’s accommodation. They are attending the same language school and spend time together every day.
They formed a band together with other refugee kids, with the local youth center providing instruments. When Kolya is on stage there, he smiles between songs. He teases Vika, who only recently started playing drums, when she can’t keep up. In the evenings, they sometimes ride bikes that people had thrown away to McDonald’s and eat fries.
Kolya says he owes it to Vika that he’s still alive. He says that when he feels her gaze, it grounds him again, brings him back to the present. Then he’s able to focus on today and push yesterday away.
Kolya has two wishes for the future. One goes like this: He wants to become an interpreter and rent an apartment, move in with Vika and marry her. He wants to do his family proud, even if they weren’t able to live long enough to see it.
The second wish is about Mariupol. Someday, Kolya would like to walk along the sea there again. He wants to show his children where he lived and where their grandparents died. He wants to see his hometown in peace and in Ukrainian hands.
Kolya knows that moment may never come. There are rumors that Russia is planning to annex the city, which would make it unreachable for Kolya. Posters are already hanging in the streets emblazoned with the words: “Russia is here forever.”
A relative still holding out in the city recently wrote Kolya that helpers had recovered the bodies of his father and sisters. They have since been buried in a mass grave. Kolya hopes to one day be able to search for them and give them a proper burial.
‘Why? Why? Why?’ Ukraine’s Mariupol descends into despair
MARIUPOL, Ukraine (AP) — The bodies of the children all lie here, dumped into this narrow trench hastily dug into the frozen earth of Mariupol to the constant drumbeat of shelling.
There’s 18-month-old Kirill, whose shrapnel wound to the head proved too much for his little toddler’s body. There’s 16-year-old Iliya, whose legs were blown up in an explosion during a soccer game at a school field. There’s the girl no older than 6 who wore the pajamas with cartoon unicorns, among the first of Mariupol’s children to die from a Russian shell.
They are stacked together with dozens of others in this mass grave on the outskirts of the city. A man covered in a bright blue tarp, weighed down by stones at the crumbling curb. A woman wrapped in a red and gold bedsheet, her legs neatly bound at the ankles with a scrap of white fabric. Workers toss the bodies in as fast as they can, because the less time they spend in the open, the better their own chances of survival.
“The only thing (I want) is for this to be finished,” raged worker Volodymyr Bykovskyi, pulling crinkling black body bags from a truck. “Damn them all, those people who started this!”
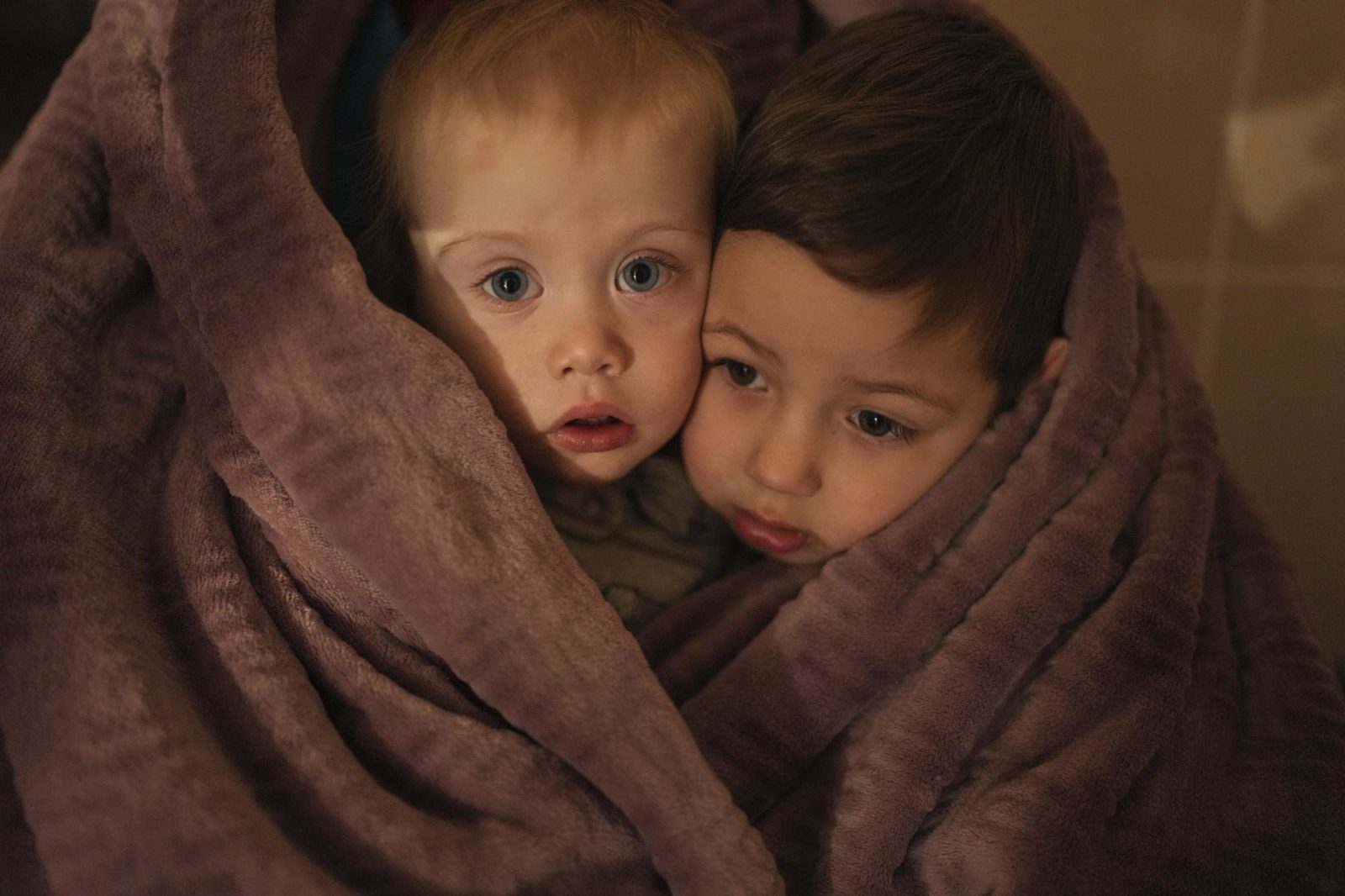
The children of medical workers warm themselves in a blanket as they wait for their relatives in a hospital in Mariupol, Ukraine, March 4, 2022. (AP Photo/Evgeniy Maloletka)

An apartment building explodes after a Russian army tank fires in Mariupol, Ukraine, Friday, March 11, 2022. (AP Photo/Evgeniy Maloletka)

A body lies covered by a tarp in the street in Mariupol, Ukraine, March 7, 2022. (AP Photo/Evgeniy Maloletka)
More bodies will come, from streets where they are everywhere and from the hospital basement where adults and children are laid out awaiting someone to pick them up. The youngest still has an umbilical stump attached.
Each airstrike and shell that relentlessly pounds Mariupol — about one a minute at times — drives home the curse of a geography that has put the city squarely in the path of Russia’s domination of Ukraine. This southern seaport of 430,000 has become a symbol of Russian President Vladimir Putin’s drive to crush democratic Ukraine — but also of a fierce resistance on the ground.
In the nearly three weeks since Russia’s war began, two Associated Press journalists have been the only international media present in Mariupol, chronicling its fall into chaos and despair. The city is now encircled by Russian soldiers, who are slowly squeezing the life out of it, one blast at a time.
Several appeals for humanitarian corridors to evacuate civilians went unheeded, until Ukrainian officials said Wednesday that about 30,000 people had fled in convoys of cars. Airstrikes and shells have hit the maternity hospital, the fire department, homes, a church, a field outside a school. For the estimated hundreds of thousands who remain, there is quite simply nowhere to go.
The surrounding roads are mined and the port blocked. Food is running out, and the Russians have stopped humanitarian attempts to bring it in. Electricity is mostly gone and water is sparse, with residents melting snow to drink. Some parents have even left their newborns at the hospital, perhaps hoping to give them a chance at life in the one place with decent electricity and water.
People burn scraps of furniture in makeshift grills to warm their hands in the freezing cold and cook what little food there still is. The grills themselves are built with the one thing in plentiful supply: bricks and shards of metal scattered in the streets from destroyed buildings.
Death is everywhere. Local officials have tallied more than 2,500 deaths in the siege, but many bodies can’t be counted because of the endless shelling. They have told families to leave their dead outside in the streets because it’s too dangerous to hold funerals.
Many of the deaths documented by the AP were of children and mothers, despite Russia’s claims that civilians haven’t been attacked.
“They have a clear order to hold Mariupol hostage, to mock it, to constantly bomb and shell it,” Ukrainian President Volodymyr Zelenskyy said on March 10.
Just weeks ago, Mariupol’s future seemed much brighter.
If geography drives a city’s destiny, Mariupol was on the path to success, with its thriving iron and steel plants, a deep-water port and high global demand for both. Even the dark weeks of 2014, when the city nearly fell to Russia-backed separatists in vicious street battles, were fading into memory.
And so the first few days of the invasion had a perverse familiarity for many residents. About 100,000 people left at that time while they still could, according to Serhiy Orlov, the deputy mayor. But most stayed put, figuring they could wait out whatever came next or eventually make their way west like so many others.
“I felt more fear in 2014, I don’t feel the same panic now,” Anna Efimova said as she shopped for supplies at a market on Feb. 24. “There is no panic. There’s nowhere to run, where can we run?”
That same day, a Ukrainian military radar and airfield were among the first targets of Russian artillery. Shelling and airstrikes could and did come at any moment, and people spent most of their time in shelters. Life was hardly normal, but it was livable.
By Feb. 27, that started to change, as an ambulance raced into a city hospital carrying a small motionless girl, not yet 6. Her brown hair was pulled back off her pale face with a rubber band, and her pajama pants were bloodied by Russian shelling.
Her wounded father came with her, his head bandaged. Her mother stood outside the ambulance, weeping.
As the doctors and nurses huddled around her, one gave her an injection. Another shocked her with a defibrillator. A doctor in blue scrubs, pumping oxygen into her, looked straight into the camera of an AP journalist allowed inside and cursed.
“Show this to Putin,” he stormed with expletive-laced fury. “The eyes of this child and crying doctors.”
They couldn’t save her. Doctors covered the tiny body with her pink striped jacket and gently closed her eyes. She now rests in the mass grave.

Oleksandr Konovalov, an ambulance paramedic, performs CPR on a girl injured by shelling in a residential area as her dad sits, left, after arriving at the city hospital of Mariupol, eastern Ukraine, Sunday, Feb. 27, 2022. The girl did not survive. (AP Photo/Evgeniy Maloletka)

The lifeless body of a girl killed during shelling at a residential area lies on a medical cart at the city hospital of Mariupol, eastern Ukraine, Sunday, Feb. 27, 2022. (AP Photo/Evgeniy Maloletka)
The same geography that for so long worked in Mariupol’s favor had turned against it. The city stands squarely between regions controlled by the Russia-backed separatists — about 10 kilometers (six miles) to the east at the closest point — and the Crimean Peninsula annexed by Russia in 2014. The capture of Mariupol would give the Russians a clear land corridor all the way through, controlling the Sea of Azov.
As February ended, the siege began. Ignoring the danger, or restless, or perhaps just feeling invincible as teenagers do, a group of boys met up a few days later, on March 2, to play soccer on a pitch outside a school.
A bomb exploded. The blast tore through Iliya’s legs.
The odds were against him, and increasingly against the city. The electricity went out yet again, as did most mobile networks. Without communications, medics had to guess which hospitals could still handle the wounded and which roads could still be navigated to reach them.
Iliya couldn’t be saved. His father, Serhii, dropped down, hugged his dead boy’s head and wailed out his grief.

Serhii, father of teenager Iliya, cries on his son’s lifeless body lying on a stretcher at a maternity hospital converted into a medical ward in Mariupol, Ukraine, March 2, 2022. (AP Photo/Evgeniy Maloletka)

Marina Yatsko, left, runs behind her boyfriend Fedor carrying her 18 month-old son Kirill who was fatally wounded in shelling, as they arrive at a hospital in Mariupol, Ukraine, Friday, March 4, 2022. (AP Photo/Evgeniy Maloletka)

Medical workers unsuccessfully try to save the life of Marina Yatsko’s 18 month-old son Kirill, who was fatally wounded by shelling, at a hospital in Mariupol, Ukraine, March 4, 2022. (AP Photo/Evgeniy Maloletka)

Marina Yatsko and her boyfriend Fedor comfort each other after her 18-month-old son Kirill was killed in shelling in a hospital in Mariupol, Ukraine, March 4, 2022. (AP Photo/Evgeniy Maloletka)
On March 4, it was yet another child in the emergency room — Kirill, the toddler struck in the head by shrapnel. His mother and stepfather bundled him in a blanket. They hoped for the best, and then endured the worst.
“Why? Why? Why?” his sobbing mother, Marina Yatsko, asked in the hospital hallway, as medical workers looked on helplessly. She tenderly unwrapped the blanket around her lifeless child to kiss him and inhale his scent one last time, her dark hair falling over him.
That was the day the darkness settled in for good — a blackout in both power and knowledge. Ukrainian television and radio were cut, and car stereos became the only link to the outside world. They played Russian news, describing a world that couldn’t be further from the reality in Mariupol.
As it sunk in that there was truly no escape, the mood of the city changed. It didn’t take long for grocery store shelves to empty. Mariupol’s residents cowered by night in underground shelters and emerged by day to grab what they could before scurrying underground again.

Serhiy Kralya, 41, looks at the camera after surgery at a hospital in Mariupol, eastern Ukraine on March 11, 2022. Kralya was injured during shelling by Russian forces. (AP Photo/Evgeniy Maloletka)

Medical workers treat a man wounded by shelling in a hospital in Mariupol, Ukraine, March 4, 2022. (AP Photo/Evgeniy Maloletka)
On March 6, in the way of desperate people everywhere, they turned on each other. On one street lined with darkened stores, people smashed windows, pried open metal shutters, grabbed what they could.
A man who had broken into a store found himself face to face with the furious shopkeeper, caught red-handed with a child’s rubber ball.
“You bastard, you stole that ball now. Put the ball back. Why did you even come here?” she demanded. Shame written on his face, he tossed the ball into a corner and fled.
Nearby, a soldier emerged from another looted store, on the verge of tears.
“People, please be united. … This is your home. Why are you smashing windows, why are you stealing from your shops?” he pleaded, his voice breaking.
Yet another attempt to negotiate an evacuation failed. A crowd formed at one of the roads leading away from the city, but a police officer blocked their path.
“Everything is mined, the ways out of town are being shelled,” he told them. “Trust me, I have family at home, and I am also worried about them. Unfortunately, the maximum security for all of us is to be inside the city, underground and in the shelters.”

People lie on the floor of a hospital during shelling by Russian forces in Mariupol, Ukraine, March 4, 2022. (AP Photo/Evgeniy Maloletka)

A Ukrainian serviceman guards his position in Mariupol, Ukraine, March 12, 2022.(AP Photo/Mstyslav Chernov)
And that’s where Goma Janna could be found that night, weeping beside an oil lamp that threw light but not enough heat to take the chill off the basement room. She wore a scarf and a cheery turquoise snowflake sweater as she roughly rubbed the tears from her face, one side at a time. Behind her, beyond the small halo of light, a small group of women and children crouched in the darkness, trembling at the explosions above.
“I want my home, I want my job. I’m so sad about people and about the city, the children,” she sobbed.
This agony fits in with Putin’s goals. The siege is a military tactic popularized in medieval times and designed to crush a population through starvation and violence, allowing an attacking force to spare its own soldiers the cost of entering a hostile city. Instead, civilians are the ones left to die, slowly and painfully.
Putin has refined the tactic during his years in power, first in the Chechen city of Grozny in 2000 and then in the Syrian city of Aleppo in 2016. He reduced both to ruins.
“It epitomizes Russian warfare, what we see now in terms of the siege,” said Mathieu Boulegue, a researcher for Chatham House’s Russia program.

People settle in a bomb shelter in Mariupol, Ukraine, March 6, 2022. (AP Photo/Evgeniy Maloletka)

A woman holds a baby in a bomb shelter in Mariupol, Ukraine, March 8, 2022. (AP Photo/Evgeniy Maloletka

People queue to receive hot food in a improvised bomb shelter in Mariupol, Ukraine, Monday, March 7, 2022. (AP Photo/Evgeniy Maloletka)

A man plays with a baby in a bomb shelter in Mariupol, Ukraine, March 6, 2022. (AP Photo/Evgeniy Maloletka
By March 9, the sound of Russian fighter jets in Mariupol was enough to send people screaming for cover — anything to avoid the airstrikes they knew would follow, even if they didn’t know where.
The jets rumbled across the sky, this time decimating the maternity hospital. They left a crater two stories deep in the courtyard.
Rescuers rushed a pregnant woman through the rubble and light snow as she stroked her bloodied belly, face blanched and head lolling listlessly to the side. Her baby was dying inside her, and she knew it, medics said.
“Kill me now!” she screamed, as they struggled to save her life at another hospital even closer to the front line.
The baby was born dead. A half-hour later, the mother died too. The doctors had no time to learn either of their names.

Ukrainian emergency employees and volunteers carry an injured pregnant woman from a maternity hospital damaged by shelling in Mariupol, Ukraine, Wednesday, March 9, 2022. The baby was born dead. Half an hour later, the mother died too. (AP Photo/Evgeniy Maloletka)

Mariana Vishegirskaya walks down stairs in a maternity hospital damaged by shelling in Mariupol, Ukraine, March 9, 2022. (AP Photo/Evgeniy Maloletka

Mariana Vishegirskaya lies in a hospital bed after giving birth to her daughter Veronika, in Mariupol, Ukraine, March 11, 2022. (AP Photo/Evgeniy Maloletka)
Another pregnant woman, Mariana Vishegirskaya, was waiting to give birth at the maternity hospital when the strike hit. Her brow and cheek bloodied, she clutched her belongings in a plastic bag and navigated the debris-strewn stairs in polka-dot pajamas. Outside the ruined hospital, she stared motionless with wide blue eyes at the crackling flames.
Vishegirskaya delivered her child the next day to the sound of shellfire. Baby Veronika drew her first breath on March 10.
The two women — one dead and one a mother — have since become the symbol of their blackened, burning hometown. Facing worldwide condemnation, Russian officials claimed that the maternity hospital had been taken over by far-right Ukrainian forces to use as a base and emptied of patients and nurses.
In two tweets, the Russian Embassy in London posted side-by-side images of AP photos with the word “FAKE” over them in red text. They claimed that the maternity hospital had long been out of operation, and that Vishegirskaya was an actress playing a role. Twitter has since removed the tweets, saying they violated its rules.
The AP reporters in Mariupol who documented the attack in video and photos saw nothing to indicate the hospital was used as anything other than a hospital. There is also nothing to suggest Vishegirskaya, a Ukrainian beauty blogger from Mariupol, was anything but a patient. Veronika’s birth attests to the pregnancy that her mother carefully documented on Instagram, including one post in which she is wearing the polka-dot pajamas.
Two days after Veronika was born, four Russian tanks emblazoned with the letter Z took up position near the hospital where she and her mother were recovering. An AP journalist was among a group of medical workers who came under sniper fire, with one hit in the hip.
The windows rattled, and the hallways were lined with people with nowhere else to go. Anastasia Erashova wept and trembled as she held a sleeping child. Shelling had just killed her other child as well as her brother’s child, and Erashova’s scalp was encrusted with blood.
“I don’t know where to run to,” she cried out, her anguish growing with every sob. “Who will bring back our children? Who?”
By early this week, Russian forces had seized control of the building entirely, trapping medics and patients inside and using it as a base, according to a doctor there and local officials.
Orlov, the deputy mayor, predicted worse is soon to come. Most of the city remains trapped.
“Our defenders will defend to the last bullet,” he said. “But people are dying without water and food, and I think in the next several days we will count hundreds and thousands of deaths.”

Anastasia Erashova cries as she hugs her child in a corridor of a hospital in Mariupol, Ukraine, March 11, 2022. (AP Photo/Evgeniy Maloletka)