The long road to a home in Europe
It is one of many boats making the crossing to Europe. On 1 August 2016, 118 migrants are rescued from the waters of the Mediterranean. They are attempting to cross from Libya to Italy, in a dinghy that is slowly filling up with water. The men – all are men – are mainly from West African countries such as Guinea, Senegal and the Gambia.
They use a migration route that is busier than ever in 2016. Due to the deal of 18 March 2016, the border between Turkey and Greece is hermetically closed. As a result, migrants are opting for the much longer crossing from Libya to Italy. Since the fall of Gaddafi and the war in Libya, human traffickers there can go about their business fairly unhindered. But it is a dangerous route, on which 4,576 people die that year – making 2016 the deadliest year in the history of migration to Europe.
At the same time, 181,436 people are rescued that year, mostly by private aid workers, and land in Italy. They dominate the news and disrupt politics, all across Europe. Most of these boat migrants are among the “fortune seekers” despised by right-wing politicians: they left their country not because of war, but because of poverty and a lack of prospects. Often, when they left, they did not intend to travel all the way to Europe. Yet that is where they would disembark in 2016.
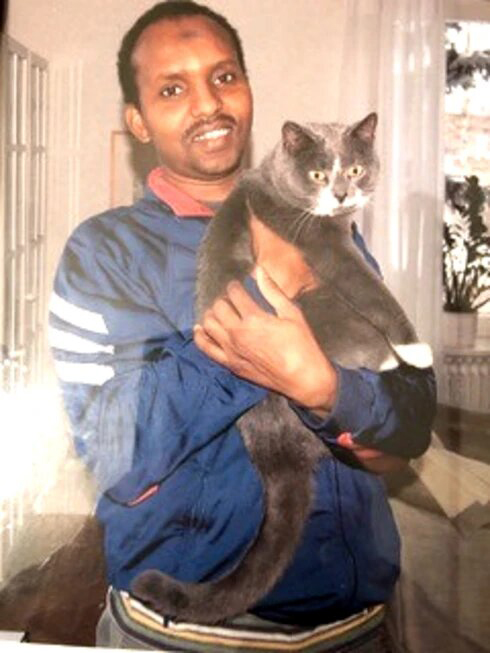
Spanish-Iranian journalist and photographer César Dezfuli, who regularly works for de Volkskrant, wants to show the people behind these numbers. He photographs all the migrants from this one boat, just after they have been rescued – their tired, drained, pained faces, scarred by the horrors in Libya, and by the journey between death and life last night.
Later he realises these pictures do not show who these people really are. Where are they now? How are they faring in Europe? And what does Europe look like through their eyes?
Dezfuli embarks on a quest. Through Facebook, he finds one of the people who was on board the dinghy. That one turns out to be in touch with some of the others, and so the photographer proceeds from one to another. He has since traced and photographed 72 of the 118 migrants. For the final eight, Volkskrant journalist Maartje Bakker joined him.
The migrants appear to have spread across large parts of Europe. They have crisscrossed the map of Europe, driven by casual contacts, numbers they have stored in their phones. Forty of them are still in Italy. More than thirty ended up in France. Others travelled on to Spain or Belgium. Some of them were in the Netherlands for a while, though none stayed here.
These men hold up a mirror to Europe. For although they are not wanted here, there appears to be plenty of work for them. In the north, they are earning very reasonable wages with jobs in industry or construction – that is, as long as their asylum procedure is ongoing, because after that they have to leave. In the south, there are also opportunities to find work without residence papers: a migrant in Italy, Spain or France can work in fruit and vegetable growing or construction, if necessary by renting someone else’s ID.
However, this is often not the end of their troubles. Life in Europe turns out to be much more complicated than many imagined. After all, those without papers have no right to exist in Europe. Yet these migrants are not giving up. They keep themselves going, send money to their families, help ensure that siblings can go to school and family members can pay for healthcare. These men, so often maligned in public discourse, show how resilient a human being can be.
And occasionally they manage to find a way up, out of that parallel reality of illegal migration, to a European life in the light of day. Perhaps through a lucky encounter with a woman, or with a Spanish or Italian boss who offers a work contract, or thanks to a lawyer who went the extra mile to arrange a residence permit.
Such an outcome is only fair, these migrants feel, after all they have endured – the only just end to their odyssey.
Neboth: “You should try to erase your memories. Don’t think about the past”
When Neboth boards the rescue ship on 1 August 2016, there is no relief or joy on his face. He is looking worried. Yes, he has reached Europe. But without his wife Joy, with whom he left Nigeria.
In his homeland, Neboth (now 36) worked as a decorator of weddings and other events. Wistfully, he thinks back to the house he grew up in, a spacious four-bedroom home. “We always put flowers outside,” he says. “I watered them and took out the bad ones in the morning.”
He has a fickle nature, sometimes calm and rational, other times angry and short-tempered. One day, he decides to leave Nigeria, hoping for a better life elsewhere. His daughter stays behind with his parents. “All the money I earned there, I spent on food,” he says. “And you don’t always have electricity in Nigeria, no good roads or schools, there are not enough hospitals. If Nigeria only had 10 percent of what Italy has, I would have stayed there.”
Neboth and his wife travel together until they, after a trip across the desert, arrive in the city of Sabha in Libya. “There they took my wife, while putting a gun to my head,” he says flatly. “If I had said anything, they would have shot me dead. It is better to stay calm, tranquilo. In Nigeria, we say: a live dog is better than a dead lion.”
Wherever he goes in Libya, he looks for his wife, but he does not find her. After six months, he decides to make the crossing to Europe alone. During the weeks before the attempt, he is living in a camp with other migrants in the dunes near Sabratha. There, he tries to recreate something of the homely life of the old days, by making himself a kind of private room. He stacks concrete blocks on top of each other and fashions a canopy out of rubbish. His room is so low that he can only lie in it, but here he can keep his things and have some privacy.
From the crossing, Neboth remembers having to take off his jacket to mop the water out of the boat. “We mopped and gave the clothes to those at the edge of the boat to wring them out,” he says.
Once in Italy, he is taken to Senigallia, a town on the Adriatic coast. After six months, he manages to get his wife’s phone number. He calls her and learns she is in Tripoli. “She was doing okay,” he says. What was she doing in Libya? “That’s not something to reveal in public.” Neboth sends his wife money for the crossing.
Neboth’s application for asylum in Italy is rejected. He travels to Switzerland, but is sent back within a few weeks. And so he is still in Italy, illegally. First he works in Sardinia, painting luxury yachts in shiny white. The ships are sold for millions; Neboth gets €700 a month for his labour. After two years, when the police start asking around about illegal workers at the shipyard, his boss tells him to leave.
Neboth ends up in Matera, a town in southern Italy, famous for its cave dwellings and early Christian churches. But that is not the Matera that Neboth gets to know. He lives in a house with other Nigerians on an industrial estate. In his room, which he rents for €200 a month, he has again tried to make himself at home. The wall is decorated with plates, and a picture of plants and butterflies. An air freshener occasionally sends out a puff of pleasant rose scent.
But right outside the front door, the raw reality begins. There are piles of stinking rubbish. Stray cats make themselves comfortable on an old car seat and a sofa.
During the day he works, still illegally, at a Chinese company that makes chairs and sofas. Neboth upholsters four or five pieces of furniture per day – Made in Italy. “These Chinese don’t care if we get sick, if we die,” he says. “If you come, you get €25 a day. And if you don’t come, nobody cares.”
Sometimes he is close to despair. “I work all day, but at night I can’t sleep,” he says. His eyes shoot back and forth restlessly. He constantly receives calls from people from Nigeria, begging him for money. He cannot understand why Italy does not give him a residence permit. “Some people have documents, but they don’t see any work they can do. They keep begging. I see work everywhere, even without documents!”
His wife made it across and these days lives in Rome. Sometimes they visit each other. She looks after an old lady with whom she lives. About the past he thinks as little as possible – the horror of what happened in Libya, the crossing, his failed attempts to build a life. “You should try to erase your memories,” he says. “Don’t think about the past. Now is now. It’s better to look to the future.”
What does that future look like? One day, he hopes to live with his wife and daughter again. “In Nigeria, we had a good life,” he says. “That is what I would like to rebuild here too. My dream is to live like any normal person.”
Oumar: “Even with a degree, my eldest brother still earned very little. That’s why I wanted to go to Europe”
It is thanks to two ruses that Oumar is on the boat that was rescued off the coast of Libya on 1 August 2016. His name was not on the list drawn up by the people-smugglers for this crossing. But he raised his hand after Diallo Boubakar’s name was called out and no one else responded. “Why the hesitation?”, he is asked. “I was dozing,” he says.
Once on the beach, he has to be inventive again. Diallo Boubakar may be on the list, but at the very bottom – and there is often no room on board for the last ones.
So once the Zodiac is in the water, and when everyone is queuing on the beach to board, Oumar hides behind the boat, in the water. Only his head rises above the waves. It is night, so no one sees him.
During the boarding there is a commotion. That is when Oumar emerges beside the boat, holds out his hands and is helped on board. Plan succeeded.
Alpha Oumar (now 28) – called Oumar for short by his friends – is from Guinea. Until the age of 20, he went to school. His father, a schoolmaster, wants him to study, to become a journalist, because he loves writing. “But I saw that my eldest brother was still earning very little with his degree,” he says. “That’s why I wanted to go to Europe.”
After some wanderings through Algeria, Morocco and Libya, he finally reaches Europe in August 2016. The Italian authorities take him to Carovigno, not far from Brindisi. Oumar, a thoughtful and deeply religious young man, assiduously attends Italian classes six days a week. Sometimes he goes to Brindisi for it, sometimes the lessons are at the reception centre. He makes rapid progress and practises his new language with the staff at the shelter.
His asylum application is rejected. Oumar knows he is faced with an important choice: which lawyer to hire? Three work at the reception centre. He chooses a man who has just started his law practice. “He will try extra hard,” he thinks, “because he has yet to establish his name.”
And indeed, he is lucky, as are about one in three asylum seekers in Italy: his application for a residence permit is granted. After one year and five months, Italy grants him asylum on humanitarian grounds, and he is allowed to work legally. Why him and not others? That is a matter for conjecture. Maybe it is the lawyer, maybe his Italian fluency, maybe the story he tells to the asylum commission. Maybe the fact that he brings along and shows all the things he has written in Italian.
In any case, it seems to be more than just a matter of chance: if you listen to the stories of a number of migrants, after a while you begin to discern a pattern. Those who did more than a few years of school in their home countries, and who had higher social status, often also seem to be able to find their way better in the European bureaucracy. Besides chance, abilities can determine fate.
Be that as it may: Oumar is crying tears of joy. He is transferred, residence permit and all, to Palagiano, the “clementine capital” of southern Italy. There he starts picking clementines and tangerines, and olives. He earns about €1,000 a month, sometimes more.
With five other migrants, he shares a house that they rent for €370 a month. For that, they have to put up with mouldy ceilings and draughty window frames. Sometimes he still writes, just for himself. He keeps his notebook in his bedside table, over which the occasional cockroach scuttles. There are stories and poems, in Italian and French.
When I was born I was black. When I grew up I was black. When the sun shines I am black. When I die I will be black. I am always black, and you are a white man. When you are born you are pink. When you stay in the sun you are red. When you are cold you are blue. When you are scared you are green. When you are sick you are yellow. When you die you will be grey. So tell me who’s a person of colour.
Oumar is not satisfied with his job in agriculture: “This is not what my father dreamed of.” He would like to have another job, an occupation where he can write – and if that’s not possible for him, then maybe for his wife?
He married her in 2019, during his only trip so far back to Guinea. He knows her from before, he would see her walking by whenever she went to school. “I love her very much,” he says, with a smile. “Every day we talk to each other.”
Oumar is trying to arrange for his wife, who is several years younger than him, to come to Italy. He is looking for a house for them together. And he hopes she will then be able to continue her studies. Literature – wouldn’t that be nice?
Modou: “It’s better to stay in one place. Then you get to understand things”
Modou sits in the boat close to the captain. He is in charge of the compass, although he had never seen such a thing before boarding. The Senegalese man has emerged as the leader of a band of migrants. It suits his character: he talks easily, to everyone, and also speaks a little Arabic, learned at Koranic school.
They sail north until they know they are far enough off the coast of Libya. “A plane flew right over us,” says Modou. “That’s when I knew we were in Italy.”
Modou (now 25) worked in Dakar as a clothes seller. Especially women’s clothes, “because women always want to look neat”. Just before he left, he visited his mother one last time, in the village where he grew up. “I didn’t tell her I was going,” he says. “But I did bring her lots of things, things like milk and rice, because I knew we wouldn’t see each other for a long time.” As soon as he crossed the border into Mali, he called her to tell her he has left. It is also the first thing he does in Italy: buy credit and call his mother. She is happy to finally hear from her son. “Thank God, she said, you are alive .”
The Senegalese knows from the start where he wants to go: to Spain, where some relatives and acquaintances live. “I always heard people talking about Spain,” he says. “I tried to listen carefully. I heard that you can live well there.”
After being plucked from the sea, he is first taken to a shelter in Italy. He ends up in the villages of Camerino and Serravalle, in the Marche region. “You couldn’t do anything there,” he says. “Just sit and wait.” He is, however, a keen attendee of Italian classes. “I want to be able to ask things,” he says. “If you don’t understand anything, you’re always scared.”
Serravalle is right in an earthquake zone. “We didn’t know that at all,” Modou notes. “In Africa, you don’t have earthquakes.” After a year, when the earth starts shaking for the umpteenth time, he decides to move on – to Spain. At the border near Ventimiglia, he pays a trafficker and travels by train to France without much trouble. Then he continues by bus to Barcelona. “I carried a book in French and pretended to be reading,” he grins. “That way, everyone would think I was a student.”
In Spain, he soon finds himself in Tàrrega, in Catalonia. Here, too, he plunges into the local language. “I already have eight diplomas,” he says. In a bar, he meets a young Spanish woman who has travelled extensively in Africa. She offers to register him with the municipality at her address. It is an important step towards recognition in Spain: migrants who have been registered for three years, and can show a work contract, are granted a residence permit. Such schemes for economic migrants also exist in other southern countries: those who work and integrate will, over time, have a chance of getting residence papers.
For Modou, the three years in Spain are now over. In the meantime, he has moved to La Fuliola, a village in the same region, among apple orchards. There, he shares an old house with as many as 20 other migrants. Its beautiful modernist floor disappears under the mattresses they sleep on at night. In summer, African migrants flock to this region to pick apples. For Modou too, it is easy to find work during those months.
But when the others leave again, he stays. “It’s better to stay in one place,” he says. “Then you understand things better, and you can get to know people.” Throughout the year, he does odd jobs for nearby farmers. They call him to feed their calves, to give them shots, to help with repairs. Sometimes he gets paid for it, sometimes not. “No pasa res,” he says. It’s no problem, in Catalan – another language he wants to master because “otherwise it would be racist”. In Modou’s words: “You have to persevere, and then you might get lucky.”
He’s right. He now has his residence permit.
Mollow: “The choice is: die here or return to Guinea”
The moment he boards the German rescue ship, Mollow’s face is serious. He is thinking about his sister. Not five minutes pass, he says, that he does not think of his sister. She has told him not to go to Europe. The crossing is too dangerous. “But I was ready to die at that moment,” says Mollow, “after everything I had been through in Libya.”
Mollow is 27, but his frizzy hair is already turning a little grey. “In my whole life, I’ve only had three or four happy years,” he says. In fact, he does not want to think back on everything he has been through. His story consists of disconnected scraps.
From the very beginning, his life was difficult: Mollow was born “out of wedlock”, the son of a Guinean father and a Sierra Leonean mother. His parents met when his father worked as a doctor in Sierra Leone during the war. Two children would be born there: a daughter, then a son.
Mollow grew up in Conakry, Guinea. He never went to school, instead selling things on the street. When he was 12, his mother died, and from then on his sister looked after him. His father’s family did not like him much, and he was even threatened by a friend of his father’s, a military man – at least, that is the story he tells. In 2011, he decides to leave Guinea: the beginning of a long quest, through Burkina Faso, Nigeria, Cameroon. Then to Algeria, after that Libya. And finally to Europe.
In Italy, he stays only two weeks before travelling on to northern Europe. “I don’t speak the language there,” he explains. “That’s why I wanted to go to a French-speaking country.” Although he never went to school, and grew up speaking Susu, he is proficient in French. He learned it along the way.
He takes the train to Rome, to Ventimiglia, to Nice. There are no checks at that point. Then straight on by train to Paris. “I don’t like France,” he says, without being able to properly explain why. He takes a Flixbus to Brussels. Arriving at one in the morning, he spends the night at Brussels North station. In the morning, he reports to the police to apply for asylum.
In Belgium, he lives in a reception centre until, after a year and a half, he is told he has no right to asylum. Mollow decides to travel on to Germany. In time, he finds work there in a car parts factory, in the Ruhr region. Proudly, he shows the wages that were deposited into his bank account, amounts around €2000. He lives in a container house all to himself. The years in Germany – those are the happy years.
Meanwhile, his sister in Guinea is in a bad way, suffering from mental illness. But with the money he earns in Germany, Mollow is able to buy medicine for her, and pay for admission to a psychiatric hospital.
Then, after four years in Germany, he loses everything. Reporting to the German authorities to extend his residence permit, Mollow is taken into custody at a detention centre. The boss of the company where he works sends a letter to the police; he would like to keep him as a labourer. To no avail. Mollow is deported to Belgium because, according to European rules, he can only apply for asylum in one country.
For a place to sleep, he now depends on friends: Guineans from the shelter in Belgium, or others he met elsewhere on his journey. This is how he ends up in Seraing, a suburb of Liège. The dominant colour there is grey – the sky, the boarded-up houses. On the horizon are the rusty remains of a steelworks. Long ago the Lion of Waterloo was cast here.
For four months now, he has been wandering from one address to another. “I’m so tired,” he keeps saying – a European would probably say depressed, but how often is that diagnosis made in Africa?
The money has run out. Mollow reveals where he sleeps: at an acquaintance’s house on the floor, in an unused corner of the shag carpet by the fireplace. He also depends on friends for food. Because he could no longer pay the bills, his sister had to leave the psychiatric hospital. She is now in a village in the care of a traditional healer, who ties her up when she has a seizure. Mollow sometimes hears her screaming over the phone.
More and more often he thinks about going back to Guinea. He is still afraid of the soldier who once threatened him, and who is now said to be high up in the army. Apart from his sister, he has nobody there. Following his mother, his father also died. “But at least I know my sister loves me,” he says.
Actually, he says, he is now at the same point as when he took the boat to Europe. “Then the choice was: suffer in Libya or die at sea. Now it is: suffer here or return to Guinea.” His eyes are filling up with tears.
Kaba: “Life is a ladder. You just have to be patient”
The boat is full, and Kaba is still on the beach. No, he thinks, this is not possible, I have to get in. But when the Guinean tries, the Libyans pounce on him. He hits back, pushes them away, and runs into the water. He dives under the boat, to the other side. There the others help him on board. He is shaking from the stress, the cold. Don’t tremble, they tell him – that way they will know it was you.
Of the crossing, Kaba remembers most of all the pain: he has to sit on one of the big screws sticking up from the bottom of the Zodiac. “In the eyes of Arabs, we blacks are donkeys, worth nothing at all,” he says.
In Italy, Kaba is taken to a shelter in Macerata Feltria, not far from the microstate of San Marino. There, he pulls out the €100 he had sewn into his pants. Since his time in Algeria, where he worked in construction, he has hidden the money there. Somehow he was not robbed of it in Libya.
Without seeking asylum in Italy, Kaba travels on to France after a few weeks, courtesy of the €100. “I don’t speak Italian, but I speak French well,” he explains. He crosses the Italian-French border on foot, along the railway tracks, ducking away when a train passes.
When he arrives in Paris, he asks around among other Africans: where can he go? A passer-by tells him to go to the 18th arrondissement, to the Porte de Clignancourt. There is a big market, where people might give him something to eat.
It is in that neighbourhood that Kaba lives on the streets, for months. During the day he stays in a park, but at night it is closed and he is condemned to the sidewalk. In the morning, he often takes the metro, line 4 from Porte de Clignancourt to Bagneux and back, sinking into a seat to try to get some sleep.
He can’t find work, you need contacts for that. So he begs for food. Sometimes he looks in a bin for discarded clothes, and sells what he finds there at the big flea market for a euro or a euro and a half.
One day, he meets a man from Ivory Coast who has squatted a house and offers him a room. “Then I slept for four days straight,” Kaba says. “I woke up, had breakfast, and fell asleep again.” The Ivorian advises him to apply for asylum. From then on, the French government gives him a living allowance, €380 a month, as long as the asylum procedure is ongoing. But after eight months, his application is rejected. Kaba receives an order stating that he must leave the country.
Again, he has to rely on chance contacts. He meets a compatriot who lives in Montauban, near Toulouse. The man is willing to give Kaba accommodation. So he ends up in the small town on the Tarn, where French people live in one neighbourhood, and Arabs and West Africans in another. “On the first day I went to the café, and there was an Arab who asked: do you want to work?”, Kaba recounts. “I said yes, of course. Then I got to work, picking apples and kiwis.”
From then on, the paid jobs string together. Always undeclared, without a contract. He currently works in construction, as a bricklayer. For every day he works, he gets €50 – a lot more that the €150 he got in Guinea for a whole month
Sometimes France is seen as a country where job contracts are gold-plated and workers’ rights are cast in concrete. In Montauban, that turns out to be only a small part of the story. France, like Italy and Spain, has a large informal economy, in which much of the work is done by migrant workers who have no papers and thus no rights. They pick the fruit, build the houses, and even keep the fast-food chains going. For a while, Kaba sold tacos, a fatty French snack, under the name of a friend who has a residence card – in return for a part of his earnings.
Kaba has not yet given up hope of getting a residence permit. There are three options. Get a work contract, together with a work permit. Conceive a French child. Or marry a French woman. He tries them all. He often goes dancing, on Saturday nights, so as to hit on women. “And I always look neat, in clean clothes,” he says.
Now, when Kaba walks down the street in Montauban, he is constantly greeting acquaintances. One offers a cigarette, which he picks with his teeth. “Ça va bien? Tranquille?” Gone are the days when he slept on the streets. “Life is a ladder,” he says, optimistically. “You just have to be patient.”
Translation by Voxeurop.
Silent Graves
Hossain Soki Walladi used to say he was born twice. The first time in Chad, a country whose regime killed his father and brother, and threw him in jail. The second time in Sweden, where he tried to build a new life. Soki was fifteen when military forces invaded his village and took him to the police station. They demanded he reveal to them the whereabouts of members of his immediate family, who were supporters of the local resistance movement. “Since I couldn’t answer their questions, they brutalised me. They beat me, put out cigarettes on my body and cut me with jagged cans and bottles,” Soki testified. After eight months of torture, he was released, only to learn that his elder brother and father had been liquidated. His mother soon passed away, and once he had provided for her funeral he fled to Libya, from where he set out for Europe by boat in 2001. When Soki arrived in Boden in northern Sweden and applied for asylum, he was seventeen. But the Swedish migration system treated him as an adult.
“This practice used to be common in our country. The Swedish authorities simply ignored what it said on Soki’s birth certificate, the only document he possessed. Also, they could not find anyone who knew the language of his tribe, so they presented him a document stating that he spoke Swahili and Arabic. Since he was illiterate and terrified, he signed it without question. That mistake meant he was labelled unreliable, and it dogged him to the very end,” says Soki’s longtime friend Anna in an interview with the Novosti weekly. She met Soki at the Red Cross in Boden, where he and her mother both worked as volunteers.
Hossain Soki Walladi 1984 – 2020. (Photo: Privatna archive)
In the following years, he learned to write and speak Swedish with the help of a local teacher, adopted a cat, Nisa, and made a wide circle of friends, with whom he travelled the whole country. He volunteered for a time as a mobility assistant for special-needs people and with the Boden municipality. Since he was popular with the clients, his supervisor once accompanied him to the migration office to help him at least obtain a work permit. But all efforts were in vain because the competent court repeatedly rejected Soki’s asylum application. At the same time, his native Chad denied him permission to return to the country. And so things continued until January 2018, when he was detained and then deported to central Africa.
“After so many years in Sweden, that was an extremely traumatic experience for Soki and all of us who knew him,” says Anna, who stayed in touch with her longtime friend.
He called her once a month, and whenever she would ask him how he was doing in Chad, he answered tersely. They last heard from each other two years ago.
“As usual, he wanted me to tell him about my family and his other friends. We reminisced about amusing situations and ended the conversation laughing. He never once told me he was on the way back to Europe. Not once. Probably he didn’t want us to worry. That’s why I got a terrible shock a few months later, when the Swedish police called and asked if I knew anyone called Soki. A person with that name on a credit card was found dead in Croatia,” adds Anna, who went on to assist the Croatian Ministry of the Interior (MUP), through Interpol, in the process of identifying the victim.
Soki Walladi’s body was pulled from the River Korana in Pavlovac, near the town of Slunj, on 28 June 2020. Although almost all the circumstances of his death remain unknown to this day, it can be assumed that he drowned after crossing into Croatia from Velika Kladuša (Bosnia-Herzegovina); presumably he aimed to return via Slovenia to the west of the European Union.
“In Boden, we still can’t believe that this happened. We often talk about him, and we miss him immensely. His small hands that made coffee and food for us, his big brown eyes, his smiles, and the affection he lavished on us,” Anna remembers her friend, whose body is buried in Skakavac, 3,000 kilometres away.
We soon found Soki’s grave at the cemetery of that village near Karlovac. Although located at the very edge of the cemetery, it can hardly be overlooked. It is covered by a mound of earth, with two tall, Islamic-style wooden grave markers protruding. The brown one has a small plaque nailed to it, with the designation 1-9-1C: here Ait and Rachid, two Moroccans whose bodies were found in the River Mrežnica in the summer of 2020, are buried beside Soki. The grave next to theirs, with the green marker and the designation 1-9-1A, is the final resting place of four more young men: Alifrom Bangladesh, Ratib from Syria, Yasser from Morocco and Eslam from Egypt. Their graves are the only ones in that part of the cemetery where there are neither flowers nor candles.
Although the crime pages of the local media and the official statistics of institutions typically treat their deaths as coincidental accidents, all seven are victims of the ruthless European migration policy that made it impossible for them to safely travel to western Europe in search of a better life, friends or relatives. This policy has criminalised those like Soki Walladi, who for various reasons, most often connected to war, were never able to obtain the necessary documents, labelling them as illegal migrants. It has also placed physical obstacles in their way – razor wire, border fences metres high, armed police patrols – and thus de facto deprived them of the right of free movement and access to international protection. In other words, it channelled them towards inaccessible border crossings, into a deadly path criss-crossed by rivers, seas, mountains, cliffs, railway tracks and minefields.

The grave of an unidentified person in Popović Brdo (Photo: Selma Banich)
Since early 2017, when the EU abruptly changed its policy towards refugees from the Near and Middle East, at least sixty-two migrants have died on the territory of Croatia: thirty-seven drowned, nine froze to death, five died in traffic accidents, two were hit by trains, two died from pulmonary oedema or lung failure, and the same number from natural causes. One person each died from falling into a cave or from a height, from an electric shock and from a land mine. In one case – a man who died this year – an autopsy has yet to be performed, so the cause of death is still unknown. In the same five-year period, a total of 140 migrants were injured, fifty-seven of them seriously and eighty-three slightly, according to the response we received from the MUP, which noted that the statistics relate to “third-country nationals who entered the Republic of Croatia illegally via the EU’s external borders and are staying in the country without permit”.
The largest number of migrants died in the Karlovac and Primorje-Gorski Kotar counties, but deaths have also been recorded in the counties of Osijek-Baranja, Vukovar-Srijem, Sisak-Moslavina, Lika-Senj, Brod-Posavina and Istria. Since their bodies are most often buried in the local cemeteries closest to the place of death, the graves are dotted through the villages around Otok, Novska, Karlovac, Duga Resa, Ozlje, Ogulin, etc. Only a few have been exhumed and returned to their country of origin, be it because some of the deceased have no family left or its members are scattered all over the world due to armed conflicts, be it because of the complex and expensive process, which, depending on the distance and the local bureaucracy, comes with a price tag of up to several thousand euros.
In the greater Karlovac area alone, where the municipal service company Zelenilo Ltd takes care of burials, thirteen migrants have been buried since January 2018. Their graves were visited by researchers involved in the project European Irregularized Migration Regime at the Periphery of the EU (ERIM). Marijana Hameršak, senior associate at the Institute of Ethnology and Folklore Research and project manager, invited artist and activist Selma Banich to join them.
“The usual practice in Karlovac County is for the names of the victims not to be indicated on the graves, even when their identities have been established. Almost all the graves are decontextualised – meaning they give no information about where the deceased came from, when they were born or how they died – and it was terrifying to realise that these people had been hounded in various ways until their death. They did not have the right to free movement, access to the asylum system and the freedom to choose the place and circumstances in which to live their lives,” Banich says and stresses that it takes their death to fundamentally change the attitude of the regime and its institutions.
“Hospitals, pathology departments, service companies, police and embassies then start dealing with their corpses, which are buried in the same ground they were chased from prior to their deaths. This is pure hypocrisy of this country, the European regime of migration control, capitalism and colonialism,” she adds.
Their first visit to the cemetery in Skakavac was quite a shock, Selma Banich says, because they were not at all certain if something was a grave or a ditch, nor how many people were buried in each. This was one of the reasons for initiating a public commemorative gesture, which resulted in the creation of “The Passage/Prijelaz”, a memorial canvas with thirty-six portraits of people who died on their migrant journey through the Balkans. Artists, social scientists, activists and other members of the Women to Women collective and the ERIM project took part in making it.
“We wanted this type of decolonial practice – a process of public mourning – to enable the local community to realise the brutality of the oppressive migration regime and oppose it,” Banich explains.

Most of the migrants died in the rivers – Dobra (Photo: Tamara Opačić)
At the same time, the MUP emphasises that the Croatian police “undertakes all in its power to save migrants in dangerous situations. […] The activities of the police to intensify the surveillance of the Croatian borders and prevent the operations of organised criminal groups do not extend exclusively to preventing illegal migration and maintaining favourable security conditions at the state border, but to protecting the lives and safety of all persons, including those who attempt to enter Croatian territory illegally,” it said in reply Novosti. The MUP also boasted of there being “too many cases to count, where the Croatian police rescued migrants whose lives were endangered by deep snow and hypothermia, by travelling in impassable mountains without proper equipment, or by injuries sustained by falling from rocks, or who had to be pulled from a river because the rugged nature of the terrain prevented them from getting out themselves – cases that have been covered by the media”.
However, Selma Banich recalls that many deaths of people on the move are a direct result of pushbacks, i.e. forceful deportations, as was the case with Madina Hussiny, a girl who was hit and killed by a train in late 2017 just after the Croatian police had forced her and her family back towards Serbia. Testimonies gathered by activists of the Border Violence Monitoring Network (BVMN) show that a large number of forcible and illegal expulsions, an estimated fifty percent of them, are carried out by the Croatian police who force refugees to enter rivers and then walk or swim back to the border of Croatia and Bosnia-Herzegovina. According to the BVMN report for 2021, such practices are most common around the village of Šturlić near Cazin, where the River Korana forms the Croatian-Bosnian border. In testimony heard in spring of 2021, five underage Afghans confirmed that the Croatian police had expelled them at that location. After apprehending the youths on Croatian territory and taking them by van to the riverbank, they ordered them to lie on their stomachs and started beating them on the legs with sticks. They then forced them to cross the border through the river, which was too deep in that part, so they had to swim. “Some people have already drowned in that spot, and there were weak swimmers among us, but we had to jump into the water so they’d stop beating us. It was terrible,” one victim of the pushback described.
“I can say from experience that the Croatian institutions are absolutely in the service of the migration regime of the European Union and its member states, which bears all the hallmarks of modern fascism. Croatia, which is currently assigned the role of guarding the area between Schengen and the EU’s external border, carries out only part of the tasks of this complex system. The problems for people on the move neither begin nor end here. The root problem is a political one: the exploitation of entire communities and resources in their countries of origin, which is why they are literally forced to flee from poverty and wars – wars ironically financed, in part, by the budget of the EU,” Banich says.
“Even if they succeed in reaching western Europe, where many of these people have family members and friends, they are made to live in a tangle of permits: residence permits, work visas and other restrictions. Most often, they are exploited as cheap labour – modern slaves who pick fruit and vegetables for our supermarket shelves,” the artist adds.
Portrait of Ahmad Kahlil Ibrahim created as part of the artistic-activist project “The Passage”
Statistics of the Missing Migrants Project, an initiative backed by the International Organisation for Migration (IOM), confirm that the murderous policies of the migration regime, compounded by the media and public’s lack of concern for the deaths of people who left their homes in search of safety, are not a characteristic of Croatia alone. Since 2014, 48,231 refugee deaths have been recorded worldwide, or at least sixteen every day. And this is a very low estimate because many bodies are never found, especially of those who drown in the Mediterranean, the mass grave of our age, in which at least 2,048 people died in 2021. European rivers, from the Marica to the Drina, Korana and Kupa, are becoming more and more deadly in recent years since the formal closure of the so-called Balkan refugee route. The IOM points out that the indifference of governments, and the resulting insufficient allocation of funds for finding and identifying bodies, is one of the key problems.
The MUP explains that this is a complex process in which several different institutions are involved, in the case of Croatia. “When a dead person is found, the police conduct an investigation, after which the body is transported to the Clinical Institute of Pathology and Forensic Medicine. A forensic examination is then conducted to determine the cause of death and the particular injuries, and the competent public prosecutor’s office is informed of the incident,” the police replied to us. The identity is determined by finding personal documents, by the people who reported the disappearance recognising the body, and by conducting dactyloscopic and DNA analyses. “In cases where data on the dead person’s citizenship is available, the Ministry of Foreign and European Affairs informs the foreign diplomatic and consular mission in Croatia, which participates in the further procedure, both in terms of notifying the family and arranging for the body to be returned. If the identity cannot be determined by the procedures mentioned, the body is kept at the forensic facility until identification is achieved,” the MUP stated. It added that, according to the data available to the border police, the identity of fourteen people who died on Croatian territory has yet to be established.
This figure would be even higher if part of the work, which should normally be done by state institutions, were not taken on by volunteers and activists who help refugees and their relatives. Information and photographs, which are crucial for finding missing persons and identifying the deceased, are most often shared through social media. In the Balkan context, the largest community is the Facebook group “Dead and Missing in the Balkans”. In one of the most recent posts, a girl from Serbia asks for news about Seif, a thirty-year-old man from Tunisia. “He disappeared somewhere between Serbia and Bosnia. He last called his family on 14 May 2019. He has a tattoo on his arm. If you have any information, please contact me via my inbox,” it says under a photo of the young man.
One such initiative allowed the identity of Ahmad Kahlil Ibrahim to be ascertained and his grave to be found. The whole life of that Palestinian was marked by war, exile and suffering. He was born in Syria, where his family had fled during the Arab-Israeli conflict. Ahmad worked as an electrician in his new home, Damascus, and started a family. But another war began, and their house was razed to the ground in 2013, so thirty-three-year-old Ahmad and his wife Rabah fled to Beirut with their three children. Due to the extreme poverty in which they lived in one of the Lebanese refugee camps, Ahmad left in the summer of 2017 for Germany, where two of his cousins live. It took him a year to reach the Bosnian-Croatian border, where he was expelled by the Croatian police. Ahmad’s next crack at the game (an attempt to cross the border) proved fatal. At the end of 2018, his body was found in the River Dobra, in the municipality of Generalski Stol. Since he had no documents with him, he was buried in the local cemetery in Lipa under the designation “Unknown male”.
Silvia Maraone (Photo: Privatna archive)
It probably would have remained that way, had not Silvia Maraone from the Italian non-governmental humanitarian organisation IPSIA (Institute for Peace, Development and Innovation) joined in the story. IPSIA has been present in the countries of former Yugoslavia since the late 1990s. Since the outbreak of the refugee crisis, Maraone has been active along the Balkan route, and in addition to providing direct psychosocial assistance she has helped refugees by publishing useful information on her blog. At the end of 2018, she shared information on people dead and missing in the Balkans. That is why, several months later, she was contacted by Ahmad’s relatives, who asked her to help.
“Since I had no information about the man, I didn’t know what to do. But at the same time, I wanted to help – I guess I thought everything would go smoothly,” Silvia Maraone recalls, who immersed herself in the case in January 2019.
She soon found an item on a local news website about a missing migrant who had fallen into the river near the Skubin Waterfall, and then she contacted several institutions on behalf of Ahmad’s family: the mountain rescue service, the Karlovac police and the Syrian consulate in Zagreb. After the body of a yet unidentified man was found in the River Dobra, she mediated in conducting a DNA analysis, and at the same time she comforted the family of the deceased, who were receiving contradictory information.
“The Red Cross joined in and supported Ahmad’s cousin from Germany in coming to Croatia and giving a blood sample. The victim’s identity was soon confirmed, but another important question still had to be answered: where was Ahmad’s body? A year later, we found out he was buried in Lipa,” Silvia tells us.

The grave of Ahmad Kahlil Ibrahim in Lipa (Photo: Tamara Opačić)
Shortly before the corona pandemic began and the borders were sealed, the Italian aid worker went to that village near Duga Resa, but since Ahmad’s grave was unmarked she was unable to find it. Since it was a Sunday, she went to a nearby church, waited until the end of mass and spoke to the priest.
“A woman, Valentina, soon joined us. She was the most diligent person I could find in that strange place and in this whole chaotic story. As a nurse who had once worked as a volunteer in Syria, she was extremely empathetic. She took me to the grave, which had a cross on it, so I asked her if there was any chance we could arrange it in accordance with Islamic tradition and add Ahmad’s name to it. Although his identity had been established months earlier, no one informed the local community, which went on to performed a wonderful gesture,” Silvia adds.
After Silvia’s visit, residents of Lipa and the surrounding villages set about rearranging Ahmad’s final resting place. They covered the bare earth with decorative pebbles, carved his name and surname, as well as the year and place of his birth and death, in a wooden board, and decorated it with flowers. Thus Ahmad Kahlil Ibrahim was given back at least a part of his dignity, which he was so cruelly divested of two years earlier at the ramparts of Fortress Europe.
Translated by Will Firth / Voxeurop.